
 It's the standard in every classroom - brightly coloured, diverse and interesting displays of children's work on each wall. I know...my mum was a teacher, and she spent ages planning topics, updating and refreshing her displays. Nothing much seems to have changed since my mum's day...every classroom I've been in recently has been the same. One was particularly well-decorated. The curtains over huge windows had large geometric shapes on them, there were things suspended from the ceiling, and I couldn't even find the door handle, there was so much stuck to the door! While such dedication to children's development is to be commended, as are the celebrations of their abilities, teachers, please spare a thought for the impact of your displays on your students with sensory processing difficulties. Sensory processing is something we all have to do in order to function. In a busy classroom, little brains have to filter out the background or unimportant sounds, sights and touch to be able to focus and get on with their work effectively. Sit for a minute yourself and listen for background sounds - the clock ticking, tapping of pencils, rattle of pipes, voices in the distance, hum of lights, and so on. Did you notice them before you actively paid attention to them? Probably not. Your brain has learned to filter them out so you can concentrate. But, imagine NOT being able to do that? Imagine hearing every sound at the same volume? How would you know what to pay attention to, or what's important?
This leads to fatigue, poor concentration, distractability, which in turn, contributes to poor behaviour and performance. So, what can you do about it? Well, there are several things you can do to maximise your students' chances of coping in a busy sensory environment:
Sometimes the pressure comes from external sources - one teacher I know was criticised during an inspection for not having enough on display. Clearly the inspector had no understanding of the sensory challenges facing those children. And it's not always possible to implement big changes, particularly if space is difficult to use flexibly and budgets are increasingly tight. But a few small changes can make a big difference to a child who struggles with sensory processing. If you'd like to understand more about sensory processing challenges and how to help, Red Robin Therapy can provide training.
 It's the summer holidays and our focus this month is play. But what do we mean by play? And why is a a balance of play activities needed? Play allows children to have fun, learn, explore, problem solve, and build social relationships. Increasingly children's 'play' consists of a high level of electronic devices and/or computer games. While I'm not knocking this (in moderation), i do believe that too much electronic time erodes into the rich variety of play opportunities that children need to become rounded, competent individuals. This article by Cris Rowan (OT) is probably more one-sided than my personal view (I think there are some benefits to technology-based play), but her strong views are interesting, and she presents the impact on sensory processing clearly. She also provides the references, so we can investigate further, should we choose to. Whatever your views on technology and play, I do agree that "movement, touch and connection to other humans" are essential to healthy development. I also think that moderation with technology is key. Let me know your views!
 It's really hard to believe that Red Robin Therapy has been going for a WHOLE year! It'd definitely true that time flies when you're having fun. Here's my year in pictures showing my significant moments, personally and professionally.
So, that's been my RRT year. There have been many more people (children and their families), organisations and events who/which have played a role in shaping things for me, so to them, and for them, I am truly grateful.
But none so much as my family!  So, your child writes like a spider has crawled across the page, they complain of a sore hand, fiddle for ages with buttons or zips, and think that excessive force compensates for anything requiring careful construction - that's before losing patience and destroying everything they've made so far. Sound familiar? It's a common issue for children with co-ordination difficulties. Time to work on those fine motor skills, right? Well, maybe not so fast. The quality of our fine motor skills are dependent on the quality of our gross motor (large movement) skills, and if we haven't achieved a good enough foundation, or are using the wrong muscles to support our fine movements, it's natural that we will struggle, get tired quickly and want to give up. Practice won't necessarily help unless we're practising the right things. We all do it - you may remember that I do a bit of weightlifting. A while back, I developed tennis elbow - inflammation of a tendon at the elbow joint - and it was sore. I couldn't lift the kettle, never mind anything else. Turned out I'd been over-using my smaller arm muscles. They eventually got fed up with this liberty and complained the only way they knew how. I had to lower the weight and retrain the larger muscles in my upper arms and back to do their job properly. It took a bit of time, but it worked. And kids with co-ordination issues are no different. If there's a weakness, their bodies try to find ways to compensate - this works for a while, but eventually school work increases, and the hand fatigue and pain becomes more regular.
While planks, push ups and balance boards are effective ways to work on core stability, they're sometimes just a bit too 'therapeutic' (boring) to keep doing with any consistency for any length of time. The good news is that there are LOADS of things you can do to make working on core stability fun.
It's all about the tools you choose. An exercise ball is a simple, but really great way to build up core strength and balance. Adding in games or toys makes it fun. You can do just about anything, and activities that need two hands become extra challenging. Make it easier by propping up a tablet to watch a movie. During floor play, get your child leaning on their elbows. It's these anti-gravity positions which work the core muscles and build strength. Have you found any similar activities which have worked well for your child? And have you noticed a difference in their fine motor skills as a result? I'd love to hear what worked for you. If you'd like an assessment or any other information about your child with co-ordination difficulties, get in touch with Red Robin Therapy.
 I'm pretty sure that all OTs set out on their career paths full of ambition and desire to do the absolute best for those in their care. They believe they can make a difference to quality of life, independence and participation - regardless of the client group they ultimately specialise with. This is certainly true for me, working with children and their families. For most of us however, at some point along the way we come to realise that doing the absolute best for our clients costs money, and most of the organisations we work within cannot meet all of the costs all of the time. Systems are in place to manage budgets - eligibility criteria, bulk procurement, recycling, reduction of non-essential spend, reduction of regular spend, freeze on spend (perhaps depending on the time of year). I'm not criticising organisations who impose these financial restraints by the way - this is a necessary evil to ensure that (in theory) resources are used fairly and wisely. But it does mean that it leaves the the OT facing a client or family with the demoralising and difficult task of having to say 'no' fairly regularly. However, what I am critical of is when statutory financial restrictions are accompanied by a lack of empowering families to source alternative means of provision for themselves. Or worse still, when families are actively blocked in their path to other solutions. I recently heard of two separate cases where managers prevented OTs from supporting families' charity applications for equipment for their child (it was considered outside their remit), although the OTs involved felt the equipment was both clinically appropriate and beneficial (very much within their remit). This makes my blood boil, if I'm honest. Not being able to access a particular item or service of choice is not something that generally happens in the absence of disability. And, it's one thing not to be able to access statutory provision - the vast majority of parents understand that resources are limited - but to be actively prevented from investigating solutions elsewhere is a disgraceful double whammy and one which is at complete odds with my core values as an OT. It's not just managers though. I've seen and heard of individual therapists who are rude, condescending or obstructive to families.
We need to be the champions of children and their families - they may not have anyone else to help in our area of expertise. We need to work closely with them, and encourage them to run new ideas past us first - this will help us identify the clinical appropriateness. If a solution happens to be inappropriate, we need to assist in finding a suitable alternative. To be pro-active and positive on behalf of families, we need to find unconventional ways to act as advocates - which might include encouraging families to complain. I'm not stirring here (I'm really not). These sort of complaints should be seen as indicators of unmet need, and should be looked at seriously by the purse-string holders. We need to provide evidence for commissioners and managers so that saying 'no' becomes much more difficult. And for us, saying no is not an option - at worst, we should be saying 'we can't do it that way, what about this way.' And there's another reason why we should be in families' corners. Increasingly, families are using the internet to find solutions; talking to each other via social media; and generally fast becoming super-informed, knowledgeable carers. Heads-up - we don't hold all the power any more - and if we're not there to help, families will do it without us. But they shouldn't have to - life is stressful enough for the family of a child with additional needs. Plus, we lose our hard-earned professional value if we're content to take this approach - and being a devalued health professional is not what I want for me or my profession. So, let's be pains in the butt for the right reasons - reminding commissioners, directors, managers and colleagues that we are here to do the best for these families. Budget restrictions are one thing, but withholding support for access to alternatives is not ever acceptable. When we become a pain in the butt for advocating on families' behalf, we can say we are doing a good job!
By the way, the two families I spoke of earlier got round their blockage. One pain-in-the-butt OT wrote a letter of support on blank paper outside of work; and one pain-in-the-butt charity agreed to accept the family's application without support from a therapist. How terribly sad that it came to that. But well done to both for being pains in the butts and putting the needs of families first.
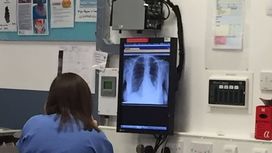
 A few weeks ago, I came across a report about research into the use of painkillers in pregnancy and an association with cerebral palsy. I said I would try to get my hands on the research article and give my take on it. So, here it is. Background CP affects approximately two in every 1000 children and is the most common condition causing movement difficulties. The inference is (and rightly so) that any knowledge which might reduce or eradicate CP has to be a good thing. Previous research The authors of this study acknowledge that no research study is perfect in design, but they point out that previous research into a possible relationship between painkillers and CP has focused on premature babies who are already at higher risk of developing CP. In addition, some studies collected the information after children were already diagnosed with CP, meaning that the accuracy of memories may have been an issue (recall bias). Finally, the underlying conditions of mothers who required painkillers were not fully accounted for, which clouded the picture (confounding variables). This study This study examined over 185,000 mums and babies from Denmark and Norway. This is a large study, and larger numbers usually mean more trustworthy results - the greater the sample, the more representative of a population any results should be. The information was collected as they went along (prospectively, thus reducing recall bias), and it was taken from the general population of mums and babies (a normative sample). Plus, they accounted for any underlying conditions that mums might have had, and they didn't include other things which might have skewed results - for example, twins, a non-surviving pregnancy, or where mums missed the first data collection. So, having dealt with the methodological issues from previous research, it seems that the authors put this study together as robustly as possible.
What did the researchers find? They found that out of all the combined data (Denmark and Norway) that almost half of mums (49%) reported using paracetamol during pregnancy, while 3% reported taking aspirin and 4% reported taking ibuprofen. They found that when children were exposed to paracetamol in the middle trimester, there was an associated increased risk of spastic CP affecting one side of the body (hemiplegia), Children who were exposed to aspirin had an associated increased risk of bilateral CP affecting both sides of the body (diplegia or quadriplegia). So, does taking painkillers cause CP? No. The authors are very clear that although these results show correlation, this does not mean causation. Think of a parallel example - we know smoking increases the risk of cancer (cause and effect), but smoking is also correlated with alcoholism - the two may happen together but alcoholism is not caused by smoking. Cause and effect is harder to demonstrate, and while the authors of this study speculate on the nervous system pathways which might make cause and effect biologically feasible, the results don't fully support the theories, and it is a long way off being known as fact. In addition... We should remember that this is a Scandinavian study, and cultural differences may not make the results applicable to us here in the UK/Ireland - we may have different patterns of prescribing and/or views on taking painkillers during pregnancy. In addition, those taking part were answering questions about use of painkillers during pregnancy, while they were pregnant. They may not have answered truthfully or they may have changed their behaviour (not taken painkillers when they otherwise might have done) just because they were in a research study (Hawthorne effect). Finally, the authors aren't 100% sure that they managed to eliminate all potential confounding variables. So, what should we take out of this? It's simply this. There appears to be an association between paracetamol and aspirin use and CP. Much, MUCH more work is needed to understand the mechanisms of nervous system development, and the study needs to be copied in similarly large numbers in other countries.
 This still makes me laugh. Me? Lifting weights?! Well, yes, it's true. I started in June 2016. But I had an absolute fear of the gym - what if I can't do it? What if people laugh? What if I hurt myself? After all, starting out as a 40-something granny I was no spring chicken! But neither was I totally decrepit, so I went along to Argos and bought a set of weights, a bar and dumbbells, and after about four weeks of being afraid to start, I eventually got stuck in to Joe Wicks' 12 week Shift, Shape and Sustain programme in my garage, living room or wherever no-one was likely to see me. I had to YouTube each exercise several times to make sure I was doing it half right. And I never knew pain like it...walking lunges were perhaps my worst - we were supposed to do them with weights and 50 for each leg. I couldn't do 50 in total with just body weight when I started!!
And, very surprisingly to me, I kept going. Literally from strength to strength. Then I outgrew the Argos weights, and had to face it. I needed a gym. Terrified, I dragged my teenage daughter along with me for a personal training session. But it was great - so I continued and she didn't! I've never really looked back - of course life throws its challenges at you. When my dad passed away last year, I struggled to get back on track, but eventually got there.
And actually, when I think about it, those are pretty good things to bear in mind for me as an OT, and for my life in general. My current training goal time-frame is the end of March, so I'll share an update with you in my April blog!!
 How's your donkeys these days? A question asked of me reasonably frequently, particularly by those who knew me before my 'farm days', and still find it hilarious! Here are my donkeys - I took this picture of Bea (short for Beatrice, in the distance) and Georgie (short for Georgina, who's ears we are looking through) and while I'd like to take credit for this artistic shot, the truth is, I had no choice in the matter! When Georgie sees me coming, she races over for a cuddle, and leans heavily against me. Bea keeps her distance, getting closer on her own terms. We've grown pretty comfortable with each other. But it's a long way from where I started. When Bea first arrived, I had no experience or knowledge of anything equine, and was petrified of this big animal who was as jittery around me as I was around her. Gradually, I learned to handle them both, grooming, worming, helping the farrier with hoof trimming, and working in close proximity to them to muck out. It's been quite a transformation!
I recently read an article about social farming which described how the charity FarmAbility enables people with autism and learning disabilities to participate in meaningful activities (a core tenet of OT) on farms. The OTnews article, and my own experience with my four-hoofed girls, led me to reflect on some of the values that working with animals can teach:
I can totally see how a farm environment would be a therapeutic environment for those who might have communication, learning or social difficulties. It's certainly a therapeutic environment for me, and as my granddaughters accompany me during my farm tasks, I know that they are learning these important values too!
 People often ask why would an occupational therapist with an established role in a reputable company, a worry-free regular income, a pension, private health care insurance, and many travel opportunities, up sticks and start her own business? And actually, when put like that, it does seem crazy - my practical self still gives off to me! The truth is, I'd always thought I'd like to run my own business, but for many years, I didn't really feel confident enough - my critical self told me I hadn't enough OT experience, practical resources, or business acumen - and I believed it. I'm not sure what changed, or when. But gradually, I realised I had two (mostly) grown-up daughters; I was granny to two beautiful granddaughters, I had racked up over 20 years of OT experience, and had worked in a business setting for 12 years. I asked myself if I still didn't feel ready, when would I consider myself able for it? The answer was now, or most probably, never.
And so, Red Robin Therapy began. When I was researching all things robin-related for my business name, I found this about my favourite little birds: The robin redbreast is a bird of Spring, a time of new growth and new beginnings. It flies into our lives on the winds of change asking us to weed our personal gardens and plant new seeds for our future. Rebirth and renewal require changes in all areas of life that have become stagnant and outdated. The robin redbreast teaches us to how to make these changes with joy in our hearts. Its song is a happy one reminding us to let go of our personal drama and learn to laugh with life. If this medicine is underdeveloped those with this totem are continually challenged by the prospects of change. Difficulties arise and emotional discord can surface. Learning how to release our attachments to the old is one of the life lessons the redbreast helps us master. How perfect! So, as 2017 nears its end and I reflect on a year of tremendous personal and professional change, I am grateful and proud. I'm grateful for the opportunity to learn new things - blogging to name just one topic! I'm grateful for the incredible number of new connections I've made in a relatively short space of time, and for the number of 'old' connections who have lent a helping hand, voice or ear when I have needed it.
Mainly though, I am proud to have met the most incredible children and families.
I can't wait to see what 2018 brings. In the meantime, have the happiest of Christmases, and the most peaceful of New Years!  So, here I am at Red Robin HQ (does that make it the Robin's Nest?), writing my first blog, and apparently stating the obvious. To explain, November 6-12 2017 is OT week, and these words are this year's theme. The challenge is for each OT to introduce themselves to those they work with, and highlight the unique benefits of the profession. Who wouldn't blog about that?! I've been an OT for nearly 24 years, and have worked with children for 23 of those. To be honest, I didn't intend to work with children, but had poorly researched a job I applied for (I got better at research as the years went on - I even got a Master's degree in it, but that's by the way). Anyway, one unexpected school for children with learning disabilities later, and a lifelong passion for paediatrics was born. The rest, as they say, is history..
Would I change being an OT?
Absolutely not. I decided I wanted to be an OT when I was 17, and I haven't looked back once! |
AuthorClare is an occupational therapist, a lifter of weights, a grandmother, a lover of dogs, pygmy goats, donkey, chickens and, of course, robins. Archives
August 2018
Categories |





























 RSS Feed
RSS Feed